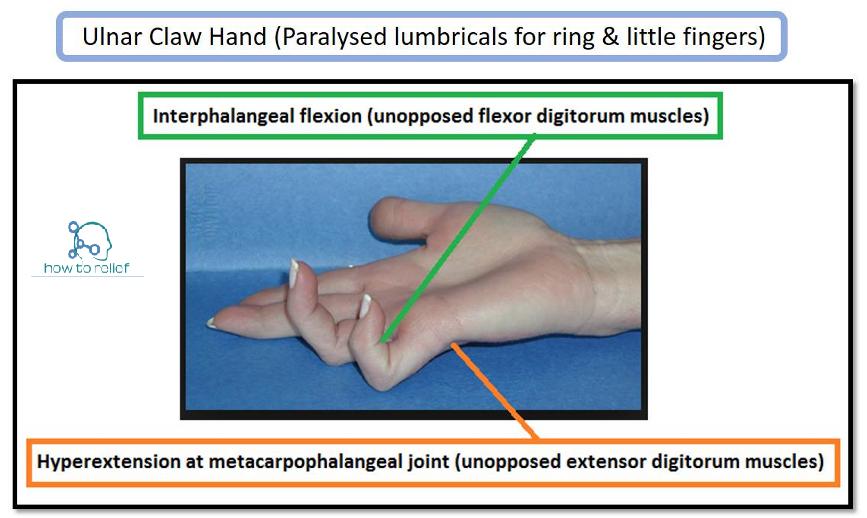
Ulnar Claw: The ulnar claw is a deformity that is seen in long-standing ulnar nerve damage at the wrist. It affects the little and ring fingers of the hand. These fingers are hyperextended at the metacarpophalangeal (MCP) joint and flexed at both interphalangeal (IP) joints.
To explain why this occurs, we need to consider the muscles that are affected by an ulnar nerve lesion at the wrist:
Medial two lumbricals: Flexes at the MCP joints and extends at the IP joints of the little and ring fingers.
Interossei: Abducts and adducts the fingers.
Hypothenar muscles: Flexes, abducts and opposes the little finger.
Adductor pollicis: Adducts the thumb.
In the ulnar claw, the important muscles to consider are the medial lumbricals. If these muscles are paralyzed, there is a loss of flexion at the MCP joints and a loss of extension at the IP joints. This leads to an imbalance between the intrinsic and extrinsic muscles of the hand – producing the claw deformity:
The MCP joints are hyperextended due to the unopposed extension from the long extensor muscles in the posterior compartment of the forearm.
The IP joints are flexed due to unopposed flexion from the long flexor muscles in the anterior compartment of the arm. The extensor muscles cannot extend at the IP joints as their energy is dissipated in hyperextending the MCP joints. The ulnar claw only occurs in the little and ring fingers, as the lateral two lumbricals are innervated by the median nerve.
Ulnar Paradox
The ulnar claw is a deformity produced by an ulnar nerve lesion at the wrist. We shall now look at what happens if the ulnar nerve is damaged more proximally – at the elbow.
In a high ulnar nerve injury, some muscles in the anterior forearm are paralyzed (in addition to the hand muscles mentioned above):

Medial half of flexor digitorum profundus: Flexes at the distal IP joints of the ring and little fingers.
Flexor carpi ulnaris: Flexes and adducts the wrist.
The ulnar claw will develop as before, but with one key difference. The flexor digitorum profundus is paralyzed, and there will not be any flexion at the distal IP joints of the ring and little fingers. Now the ulnar claw only consists of hyperextension at the MCP joints and flexion at the proximal IP joints. This produces a much less evident claw hand.
This is known as the ‘ulnar paradox‘ – you would expect a more debilitating injury to produce a more pronounced deformity, but in fact, the opposite occurs.